

Telehealth weight loss program options have fundamentally transformed the way millions of people approach obesity treatment — moving care out of crowded waiting rooms and into the palm of your hand. In 2026, these digital-first platforms are no longer a workaround or a compromise; they represent the gold standard of scalable, medically supervised obesity care. With global obesity rates projected to affect 51% of the world’s population by 2035, understanding how to navigate this evolving landscape is not just smart — it is essential.
Whether you are exploring your very first online weight loss solution or looking to switch from a compounded medication to a branded FDA-approved protocol, this guide will walk you through clinical benchmarks, real-world outcomes, cost structures, safety standards, and the behavioral strategies that separate programs that truly work from those that simply take your money. For a broader clinical foundation, start with the Weight Loss: The Complete Clinical Guide for 2026.
Before we dive in, one thing worth clarifying upfront: the phrase “telehealth weight loss” covers a wide spectrum. At one end, you have app-based platforms that mail you a prescription with minimal oversight. At the other, you have fully integrated digital clinics staffed by board-certified obesity medicine specialists, registered dietitians, and behavioral health coaches who work together in a coordinated care model. Knowing the difference — and knowing how to evaluate it — is the first and most important skill any patient can develop before enrolling in any online weight loss program.

Table of Contents

Why the Telehealth Model Has Become the Standard of Care
Not long ago, managing your weight medically meant scheduling an appointment, waiting weeks to be seen, and then navigating a referral process just to access the tools that could actually help. That bottleneck is gone. A modern telehealth weight loss program removes every unnecessary barrier between a patient and a licensed obesity medicine specialist.
The convenience factor is obvious — but convenience alone does not explain why clinical outcomes from telehealth platforms now rival those seen in phase 3 drug trials. The real driver is access. When patients can connect with a provider from home, engage with behavioral coaching tools daily, and have medication delivered to their doorstep, adherence skyrockets. And in chronic disease management, adherence is everything.
For those who are simultaneously managing their journey from home, the Weight Loss at Home article offers complementary strategies that integrate seamlessly with a telehealth program.
The 2026 Market Shift: From Compounded to Branded Medications
One of the most significant developments in the online weight loss space this year was the formal transition away from compounded GLP-1 medications toward branded, FDA-approved options. A landmark moment came in March 2026, when Novo Nordisk struck an agreement with Hims & Hers to provide branded Ozempic and Wegovy at self-pay prices that are actually competitive.
This matters enormously. Compounded medications — while cheaper — were produced outside the standard FDA quality controls that govern manufacturing, dosing precision, and purity. For patients trying to loss weight safely and effectively over the long term, branded medications represent a far more reliable clinical foundation.
Current platforms now offer a full spectrum of GIP and GLP-1 receptor agonists, including semaglutide (marketed as Wegovy and Ozempic) and tirzepatide (Zepbound). These molecules mimic naturally occurring gut hormones that regulate appetite, slow gastric emptying, and improve blood sugar control. The arrival of the first oral GLP-1 approved for weight management — the Wegovy pill — has made it even easier for patients who struggle with self-injection to participate in medically supervised care.
Clinical Efficacy: What the Data Actually Shows
When you are choosing an online weight loss program, marketing language is everywhere. What cuts through the noise is data.
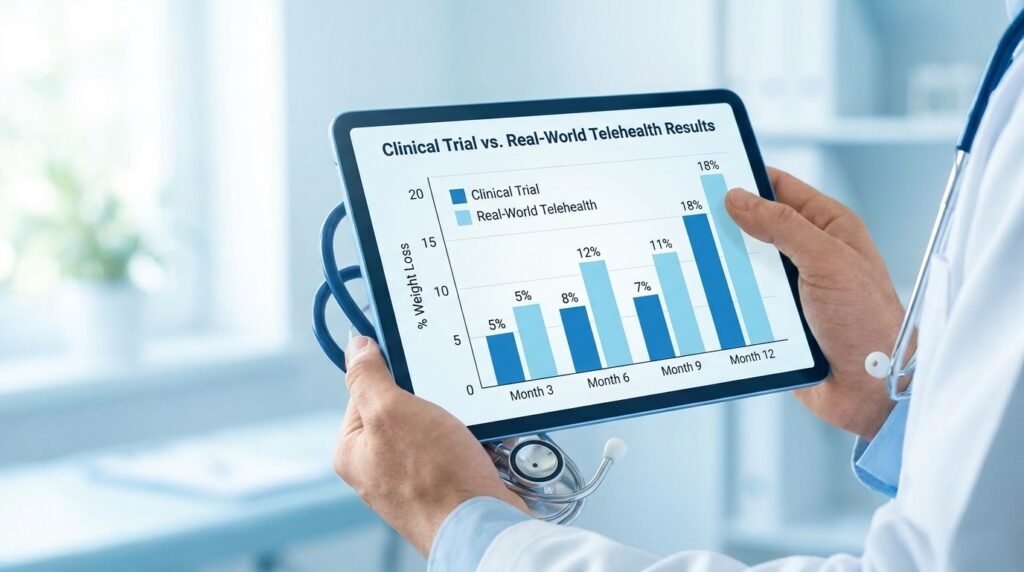
Semaglutide (Wegovy): In the landmark STEP 1 trial, patients using once-weekly semaglutide injections achieved a mean body weight reduction of 14.9% over 68 weeks. Real-world data collected from telehealth cohorts between 2024 and 2025 showed a mean reduction of 13.8% at 12 months — a remarkably close correlation that validates the telehealth delivery model as clinically sound.
Tirzepatide (Zepbound): The SURMOUNT-1 trial reported a mean weight reduction of 20.9% at maximum doses. Real-world self-pay cohorts, however, showed a mean of 12.5% — a gap largely attributed to the economic difficulty of titrating to the highest dose when paying out-of-pocket. For patients who can reach the maximum tolerated dose, tirzepatide remains the most potent single agent available to loss weight in 2026.
Diabetes Prevention: A three-year study sponsored by Eli Lilly demonstrated that tirzepatide reduced the risk of progression from pre-diabetes to type 2 diabetes by 94% — a finding that reframes these medications not just as weight loss tools but as transformative metabolic interventions.
One data point every patient must understand is the physiological plateau. Research consistently shows that weight loss velocity peaks in the first three months (approximately 1.07 lbs per week) before declining significantly between months 12 and 15. This is not failure — it is physiology. Understanding this transition helps patients stay committed through what can feel like a frustrating plateau. For a full breakdown of how to sustain momentum through this phase, see How to Lose Weight.
The Behavioral Layer: Why Medication Alone Is Never Enough
Perhaps the most underreported truth in the online weight loss world is this: GLP-1 medications are powerful, but they are not a complete solution on their own. The behavioral layer — tracking, coaching, community, and habit formation — is what separates patients who maintain their results from those who regain weight the moment they stop the medication. Every credible telehealth weight loss program recognizes this and builds behavioral infrastructure into the clinical model, not as an optional add-on but as a core component of treatment.
A systematic review and meta-analysis published in the Journal of Medical Internet Research examined what happens when patients combine self-monitoring smartphone apps with professional health coaching. The results were striking:
- Weight loss improved by an average of 2.15 kg beyond medication alone
- Waist circumference decreased by an additional 2.48 cm
- Daily calorie intake dropped by an average of 128.30 kcal
- Triglyceride levels and HbA1c both improved meaningfully
WeightWatchers Clinic’s internal data reinforces these findings even more dramatically. Med+ members who actively engaged with behavioral coaching tools lost 29.1% more body weight over 12 months compared to members who relied solely on medication. This is not a marginal difference — it is a clinical distinction that should shape how every patient evaluates an affordable telehealth weight loss option.
For patients who want to understand the nutritional science underpinning these behavioral recommendations, the role of nutrition in weight management provides an evidence-based deep dive.
Financial Navigation: What Telehealth Weight Loss Actually Costs in 2026
Cost has historically been one of the greatest barriers to accessing medically supervised obesity treatment. In 2026, the landscape has shifted — but it remains complex. Here is what you need to know.
Medicare Part D: The $2,100 Out-of-Pocket Cap
Patients with Medicare drug coverage (Part D) now benefit from a landmark policy change: a hard annual cap of $2,100 on out-of-pocket drug costs. Once that ceiling is reached, you pay nothing further for covered medications for the remainder of the year. For patients on high-cost GLP-1 medications, this cap is genuinely life-changing.
Self-Pay Pricing Tiers (2026)
For those without insurance coverage, affordable telehealth weight loss access is increasingly available through transparent, tiered pricing models:
- LillyDirect: Zepbound starts at $299/month for the 2.5 mg starting dose, rising to $399 for 5.0 mg and $449 for higher doses — all branded, FDA-approved tirzepatide direct from the manufacturer.
- WeightWatchers Clinic: Med+ membership begins at just $25 for the first month, then $74/month thereafter (medication cost billed separately).
- Mochi Health: Compounded semaglutide from $99/month; compounded tirzepatide from $199/month — among the lowest entry points currently available.
Many telehealth platforms now employ dedicated insurance coordinators to handle prior authorizations, appeal denials, and maximize coverage — a service that can easily save patients thousands of dollars annually. For a curated comparison of the top Weight Loss Programs by price and clinical model, visit that resource before making your decision.

Top-Ranked Telehealth Weight Loss Programs for 2026
Forbes Health conducted a rigorous analysis of 41 data points across the leading platforms to identify the best online weight loss programs available this year. Here is what they found:
WeightWatchers Clinic — 5.0/5 | Best Overall The gold standard for integrated care. WeightWatchers combines obesity medicine specialists, registered dietitians, and an unmatched community support infrastructure. It is the top recommendation for patients who want a comprehensive, medically supervised experience designed to loss weight and maintain it.
Ro — 4.5/5 | Best for Provider Communication Ro earned its ranking through unlimited provider messaging and a dedicated insurance team that actively works to secure coverage for patients. For anyone who values responsive, ongoing clinical support, Ro sets the bar.
Mochi Health — 4.3/5 | Best User Experience Mochi’s platform is praised for its intuitive design, AI-powered pricing chatbot, and efficient virtual visit scheduling. It is the top pick for patients who value a seamless digital experience alongside affordable telehealth weight loss pricing.
Remedy Meds — 4.3/5 | Best Customer Service With direct shipping to all 50 states and highly rated patient support, Remedy Meds is an excellent choice for patients in rural or underserved areas who need reliable delivery and consistent care.
PlushCare — 4.1/5 | Best Clinical Credentials PlushCare connects patients with board-certified physicians licensed in all 50 states. For patients who prioritize physician-led care and rigorous credentialing, it is a standout option.
Consumer Safety: How to Identify a Legitimate Telehealth Provider
The explosive growth of the online weight loss market has unfortunately created space for bad actors. For anyone determined to loss weight safely and with proper clinical oversight, learning to identify a legitimate provider is a skill that protects both your health and your wallet. Before handing over your credit card or your health history, verify these five compliance standards:
- State licensing: The prescribing provider must hold an active license in the state where you are physically located at the time of the visit — not where the company is headquartered.
- Synchronous consultation: A legitimate program requires a real-time video consultation, not just a text questionnaire. This is a regulatory and ethical requirement for establishing a valid physician-patient relationship.
- Lab review: A credible telehealth weight loss program will request and review recent bloodwork before prescribing — particularly for patients with cardiovascular risk factors or a history of thyroid conditions.
- Licensed pharmacy fulfillment: Medications must ship from a pharmacy licensed in your state.
- No pre-prescription payment for drugs: It is illegal — and a major red flag — for any platform to collect payment for medication before a provider has issued a prescription.
Avoid any platform that promises automatic approval, skips the medical intake, or fails to offer ongoing clinical follow-up. A legitimate affordable telehealth weight loss service treats you as a patient, not a transaction.
Gender-Specific Outcomes: What the Data Reveals
Real-world data from telehealth platforms has surfaced a striking gender divergence in how patients experience GLP-1 therapy — findings that have important implications for how programs should personalize care. These insights are shaping how the best online weight loss platforms now design their intake processes and titration protocols by gender.
Women represent approximately 80% of online weight loss telehealth enrollees and are significantly more likely to be classified as “major responders” — achieving more than 20% total body weight loss. The female major-responder rate sits at 29.8% compared to just 5.9% for men.
Men, however, demonstrate higher engagement frequency — attending more virtual visits (13.5 vs. 12.7 on average) and reaching out to providers more often. Researchers suggest this reflects a behavioral compensation pattern: men who experience slower physiological progress tend to troubleshoot more actively rather than disengage. Understanding these differences allows both patients and providers to set more accurate expectations and tailor support accordingly. An affordable telehealth weight loss program that ignores gender-specific physiology is leaving meaningful clinical value on the table — and potentially setting male patients up for discouragement when they compare their early results to population-level data skewed by female major-responders.
The Long Game: Moving From Induction to Maintenance
If you are using a GLP-1 medication to loss weight, you must plan for the long term from day one. The biology is unambiguous: when GLP-1 medications are discontinued, the hormonal signals that were suppressing appetite return to baseline, and weight regain is common — often rapid. Patients who loss weight rapidly in the first three months and then abruptly discontinue their medication without a tapering or maintenance plan are at the highest risk of significant regain within six to twelve months.
This is not a character flaw or a lack of willpower. It is pharmacology. Just as a patient with hypertension continues their medication to maintain controlled blood pressure, a patient using GLP-1 therapy for obesity management is treating a chronic condition that requires ongoing intervention.
A high-quality telehealth weight loss program will help you:
- Titrate intelligently: Finding your minimum effective dose — the lowest dose that maintains your target weight — reduces long-term cost and side effect burden.
- Build metabolic resilience: Prioritizing protein intake, resistance training, and sleep quality protects lean muscle mass during weight loss and makes maintenance more physiologically sustainable.
- Track body composition, not just weight: The scale is a blunt instrument. Tracking fat mass versus lean mass gives a far more accurate picture of metabolic health progress.
- Plan transitions proactively: If cost, insurance changes, or side effects require a medication change, having a plan ready prevents the reactive decisions that lead to regain.
For patients who want to accelerate results safely during the induction phase, the evidence-based strategies in how to weight loss quickly are worth reviewing alongside your clinical protocol.
Building a Sustainable Approach: Lifestyle as the Foundation
No telehealth weight loss program — regardless of how sophisticated the technology or how potent the medication — can override a lifestyle that actively works against you. The research is consistent: the patients who achieve and maintain the most significant results are those who use medication as a lever, not a crutch. If your goal is to loss weight and keep it off, lifestyle architecture is the non-negotiable foundation beneath the pharmacology.
What does that look like in practice?
Nutrition: GLP-1 medications reduce appetite, but they do not select for nutritional quality. Patients who prioritize protein (typically 0.7–1.0 grams per pound of body weight), limit ultra-processed foods, and eat adequate fiber achieve better body composition outcomes than those who simply eat less of their existing diet. Any credible online weight loss program will assign you a structured dietary framework — not just a calorie target — within the first weeks of treatment.
Movement: Resistance training during active weight loss is non-negotiable for preserving muscle mass. Even two sessions per week make a measurable difference in the ratio of fat-to-lean mass lost. Patients who loss weight without a concurrent resistance protocol tend to experience a metabolic slowdown that makes long-term maintenance significantly harder.
Sleep: Chronic sleep deprivation elevates ghrelin (the hunger hormone) and suppresses leptin (the satiety signal) — directly undermining the very mechanisms GLP-1 medications are enhancing. Prioritizing seven to nine hours of quality sleep is a clinical intervention in its own right, and any affordable telehealth weight loss program that overlooks this is leaving meaningful results unrealized.
Stress management: Cortisol dysregulation from chronic stress promotes visceral fat storage and drives compulsive eating behaviors. Behavioral support — whether through coaching, therapy, or structured mindfulness — is part of what makes the best online weight loss programs more effective than medication alone. When you sign on with a quality telehealth provider, ask specifically what behavioral support infrastructure looks like — not as a courtesy feature, but as a clinical component you should actively use.
For a comprehensive roadmap to Healthy Weight Loss that integrates all of these pillars, that resource offers a well-rounded complement to your clinical program.
Conclusion: Choosing the Right Program in 2026
The telehealth weight loss program landscape in 2026 is more sophisticated, more regulated, and more effective than at any prior point in its history. Real-world data now confirms that patients using medically supervised online weight loss platforms achieve outcomes that closely mirror what was once only possible in clinical trial settings — when they engage fully with both the medication and the behavioral support layer.
The key decisions come down to three things: the medication (branded vs. compounded, semaglutide vs. tirzepatide), the platform (level of clinical oversight, communication access, and behavioral tools), and the financial model (insurance, self-pay tiers, or Medicare Part D coverage under the new $2,100 cap).
Whichever path you choose, prioritize platforms that treat you as a patient in an ongoing clinical relationship — not as a subscriber in a subscription. The best affordable telehealth weight loss programs invest in your outcomes, not just your enrollment. They will adjust your dose when you plateau, check in when your labs show a red flag, and help you build a maintenance plan before you need one.
The tools to loss weight effectively and sustainably have never been more accessible. Every year, the clinical evidence base expands, the regulatory framework tightens, and the pricing models become more patient-friendly. A high-quality online weight loss program today gives you access to the same class of interventions that wealthy patients have been paying out of pocket for at boutique clinics for years — at a fraction of the cost and with considerably more flexibility.
The question in 2026 is not whether a telehealth weight loss program can deliver results — the data confirms that it can. The question is whether you choose a program designed to support you through the entire journey, from the first dose to long-term metabolic health. Look for transparent pricing. Look for licensed providers. Look for behavioral support. And above all, look for a program that helps you loss weight in a way that is clinically sound, financially sustainable, and built around your life — not around a one-size-fits-all protocol that ignores who you actually are.
That distinction is everything.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult with a healthcare professional before starting any weight loss program. Please seek proper guidance to ensure your safety and well-being. The information on this site is not intended to replace professional clinical consultation.
Pingback: minoxidil biological mechanism